The Human Diagnosis that Shatters Modernism
Note: This section is designed for—but not restricted to—researchers.
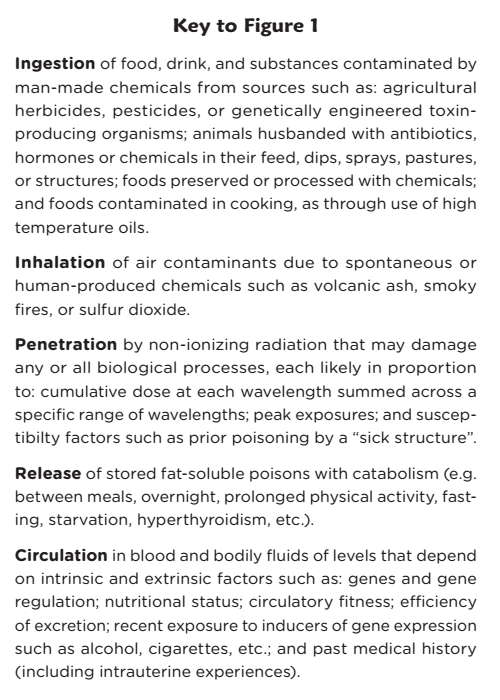
You are swimming in a sea of irritants that trigger the immune system and promote allergies. In medical literature, you can find studies that show sulfur dioxide from car exhaust to be a catalyst for the development of asthma, which is now viewed and treated as an inflammatory response. In “alternative” literature, you can find the diagnosis of leaky bowel which—with popular books such as Wheat Belly—point to a similar catalysis of inflammation by ingested toxins. On the fringe, many patients are coping with radiation poisoning in the electromagnetic range. Thus, regardless of the route of exposure, you may—if not very careful—take in chemical irritants or non-ionizing radiation that does you active harm, and that may overcome your body’s compensatory mechanisms now or in the future, according to your dose and susceptibilities.
The medical system relies heavily on premodern fatalism and modern over-management. Discovery is rare; more common are desensitization to new conditions, suppression of symptoms, and chemical attack on living systems that may in itself do more harm than good. This is how medicine can “conquer” many communicable diseases. While occupational medicine can detect and mitigate harm done by high exposures, no branch of medicine is prepared to deal with the consequences of ambient poisoning. Preventative medicine and public health practitioners struggle to use prevention as cure, but modern methods depend on reasoning backward from disease and death rather than forward from hazards. One reason for this is that the early consequences of chronic poisoning are protean, elusive, and subject to change. You can see this in the difficulty of defining pre-diabetes or estimating the adverse impacts of obesity. Another is that one size does not fit all; the consequences of exposure are impacted by intergenerational and personal factors and by the rapid increase in multiple exposures—what you can view as the ever-changing and cumulative poison cocktail. All of these issues call for new formulation of ailments, causal thinking, and investigative methods. Fortunately, these problems have not gone unnoticed by the loyal opposition—that is, by medical thinkers who have been integrating medicine and preparing for emergence.
Preventive Cure
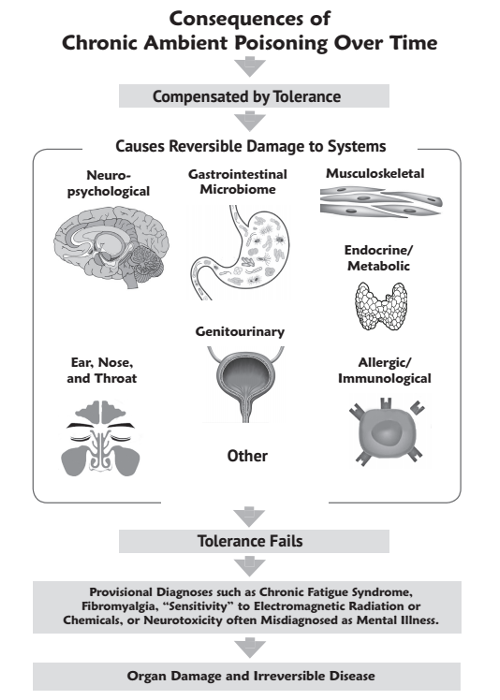
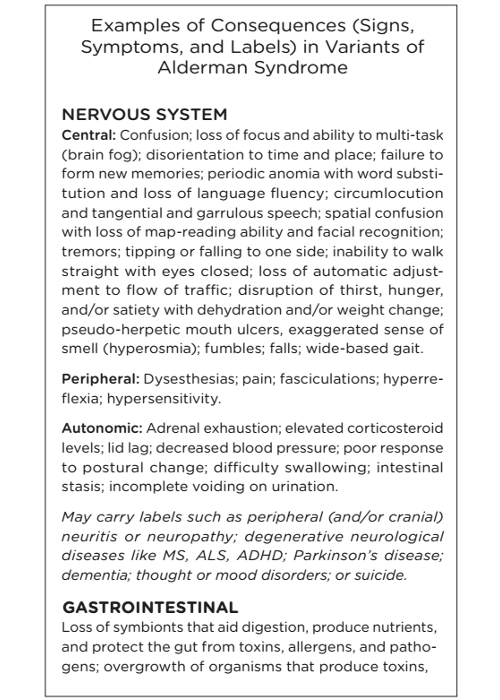
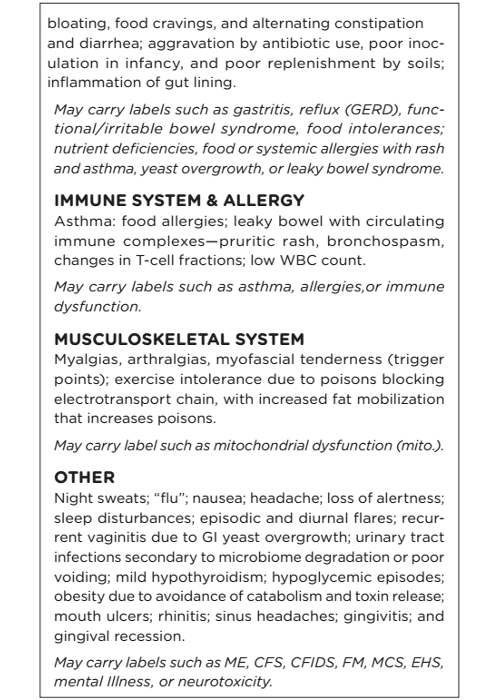
In chronic ambient poisoning (CAP), also called Alderman syndrome, poisoning is continuous or recurrent with peaks of varying magnitude and produces signs and symptoms that may be disabling for years before the detection of any consequent final common pathway diseases. As a diagnosis, CAP thus moves the focus of research and intervention up the causal web from death and end-stage disease to primary causes. Thus, it enables preventive cure. Due to the diversity of poisons; the diversity of genes and their impacts on metabolism; the diversity of end organ effects resulting from the poisoning process; and the diversity of lifetime combined and cumulative dosages of various poison “cocktails,” each case must be defined and investigated with an “N-of-1” study in which suspected causes are eliminated for long periods in hopes of effecting detoxification and resultant recovery and cure (see Medical Detective).
Chronic Exposure
With the ubiquitous dissemination of natural and synthetic chemicals and radiation that poison life and contribute to vitacide (e.g. extinction of evolved life), humans have developed new ailments analogous to those in other species such as birds, bees, amphibians, and insects. Since the discovery of fire, and earlier, humans have been creating toxins that cause illness. One premodern example is nasopharyngeal cancer due to the combination of indoor smoky fires with Epstein-Barr virus exposure; another is lung disease, an occupational ailment of stonemasons, millers, bakers, coal miners, and others. The radical experiment of modernity has led to many new chronic illnesses in workers, including: jaw cancer in women who painted clock hands with radium, testicular cancer in chimney sweeps, lung cancer and asbestos in dock workers, and cognitive delay in children due to lead paint.
Now that poisons have been disseminated through the wild and modified world, chronic and cumulative low-dose exposure is causing new kinds of ailments that cannot be comprehended within the modern worldview. These new hazards are also increasing rates of certain long-standing diagnoses. This applies to an unknown proportion of patients, perhaps especially those with disabling neurological conditions. Very little is known, partly because modern ideas and methods are integral to the problems of late modernity and thus unsuited for creating solutions (see “Evidence-Based Medicine” in This Idea Must Die). Examples of this lack of traction include almost all studies to date of ME/CFS and of the health effects of non-ionizing radiation.
Diagnosis
All diagnosis is clinical, and therefore problematic with respect to a system that places uncertainty and ambiguity squarely in the Jungian shadow—that is, that which we ignore. In the case of medicine, relegation to shadow entails referring patients to psychiatry for drugging that stops complaints. Doctors who are independent-minded, curious, and open may be better prepared to look into the shadows, in which case they will be stymied by constellations of symptoms that are not in the textbook and that make no sense within the modern frame. A clinically-derived causal model linked to etiopathogenesis, like the one presented here, can come only from the type of clinical research that has fallen out of favor and been quashed by false ideas of time efficiency (e.g. doing what is expected as quickly as possible while thinking as little as possible). This and information overload have obstructed development of a useful diagnostic gold standard. There is thus no metric against which to evaluate potential biomarkers as diagnostic tests. This is a problem as most “markers” have little or no diagnostic utility. Fortunately, the N-of-1 self-study reported here has provided an etiopathogenic model that is deterministic in one patient and that can serve as a model for further N-of-1 studies by other patients and their doctors.
Etiopathogenic Model
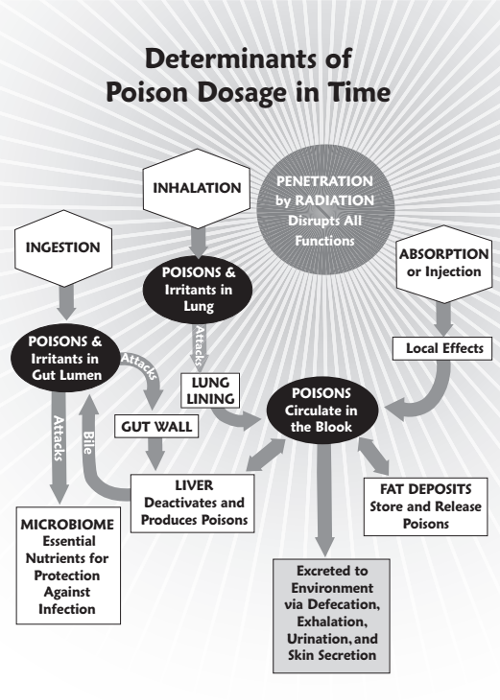
Poisoning in Time
Consequences over Time